
Syndrome Description
Learn more about M-CM
While a genetic marker for M-CM has been recently identified, diagnosis can usually be made based characteristics seen in an individual. In 2015, a clinical genetic test became available for the first time, so cases with unclear diagnosis based on clinical signs can undergo genetic testing. Genetic testing guidance is available on our Genetic Testing Recommendations page.
Four different diagnostic criteria have been proposed to diagnose M-CM and are described below. The first two criteria were developed prior to the name change to M-CM and refer to cutis marmorata or cutis marmorata telangiectatica congenita as key features of the condition.
Even with use of clinical diagnostic criteria, an individual’s entire clinical picture must be considered. Providers with personal expertise in evaluating those with M-CM and who have familiarity with the variability of the clinical diagnosis are poised to have greater success in making an accurate diagnosis.
The first author to propose diagnostic criteria for M-CM was Robertson et al. in 2000. This criteria suggested that a diagnosis of M-CM could be made in an individual if they had congenital macrocephaly AND CMTC with at least FOUR of the following features:
Shortly after the Robertson criteria were published, Franceschini et al. reported two cases of M-CM in whom the characteristic vascular changes of the skin faded over time. This was the first paper to clearly make this observation. Franceschini felt that the presence or absence of CMTC/capillary malformation was not necessarily required to make a confident diagnosis since in some affected individuals, this finding was age-dependent and might resolve with time. Therefore, Franceeschini’s criteria stipulated that a diagnosis of M-CM should be considered in an individual who has macrocephaly AND at least TWO of the following features:
The third criteria presented by Wright et al. in 2009 presented a modification of the two aforementioned criteria and basically combined aspects of both into a new proposed method of diagnosing M-CM. These authors retained the combination of macrocephaly AND capillary malformation(s) occurring anywhere on the body as mandatory features with the required presence of a specific number of minor features similar to those proposed by Robertson. However, Wright’s criteria are less restrictive than those of Robertson and they state an individual must have at least TWO of the following in addition to the previously mentioned mandatory features:
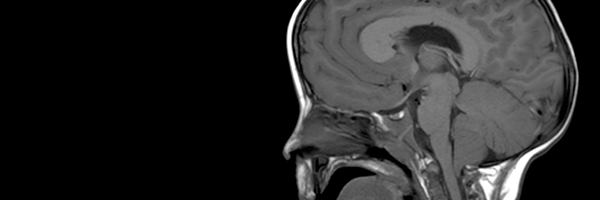
A fourth diagnostic criteria was proposed in 2010 by Martinez-Glez et al. and suggests the presence of at least 3 major and two minor criteria. This criteria takes into account the fact that abnormalities on neuroimaging are extremely common in M-CM and represent a recognizable pattern of abnormalities:
|
Major (at least 3) |
Minor (at least 2) |
|
|
Unlike the three prior proposed criteria, the paper published by Martinez-Glez et al. is unique in that the authors attempted to test their criteria against previously reported cases to demonstrate its ability to make an accurate clinical diagnosis of M-CM. The authors were able to diagnose 94% of 136 previously reported cases of M-CM using their criteria. This suggests that to date, it may be the best set of clinical criteria available to aid in the diagnosis of M-CM.
Order brochures or download a PDF
Guidelines from published research literature
Guidance for clinical genetic testing

Explore the results of a patient survey conducted in 2012

Explore the research literature related to M-CM

An extensive list of resources